高效考點與陷阱
- 大腦皮質功能定位是必考題型:Broca's area(BA 44, 45)在優勢半球的下額回,管「說」;Wernicke's area(BA 22)在後上顳回,管「懂」。損傷後 Broca's aphasia 能懂不能說(non-fluent),Wernicke's aphasia 能說不能懂(fluent but meaningless)。弓狀束(arcuate fasciculus)連接兩區,斷了 → conduction aphasia,聽懂也能說,就是「覆述」特別差。
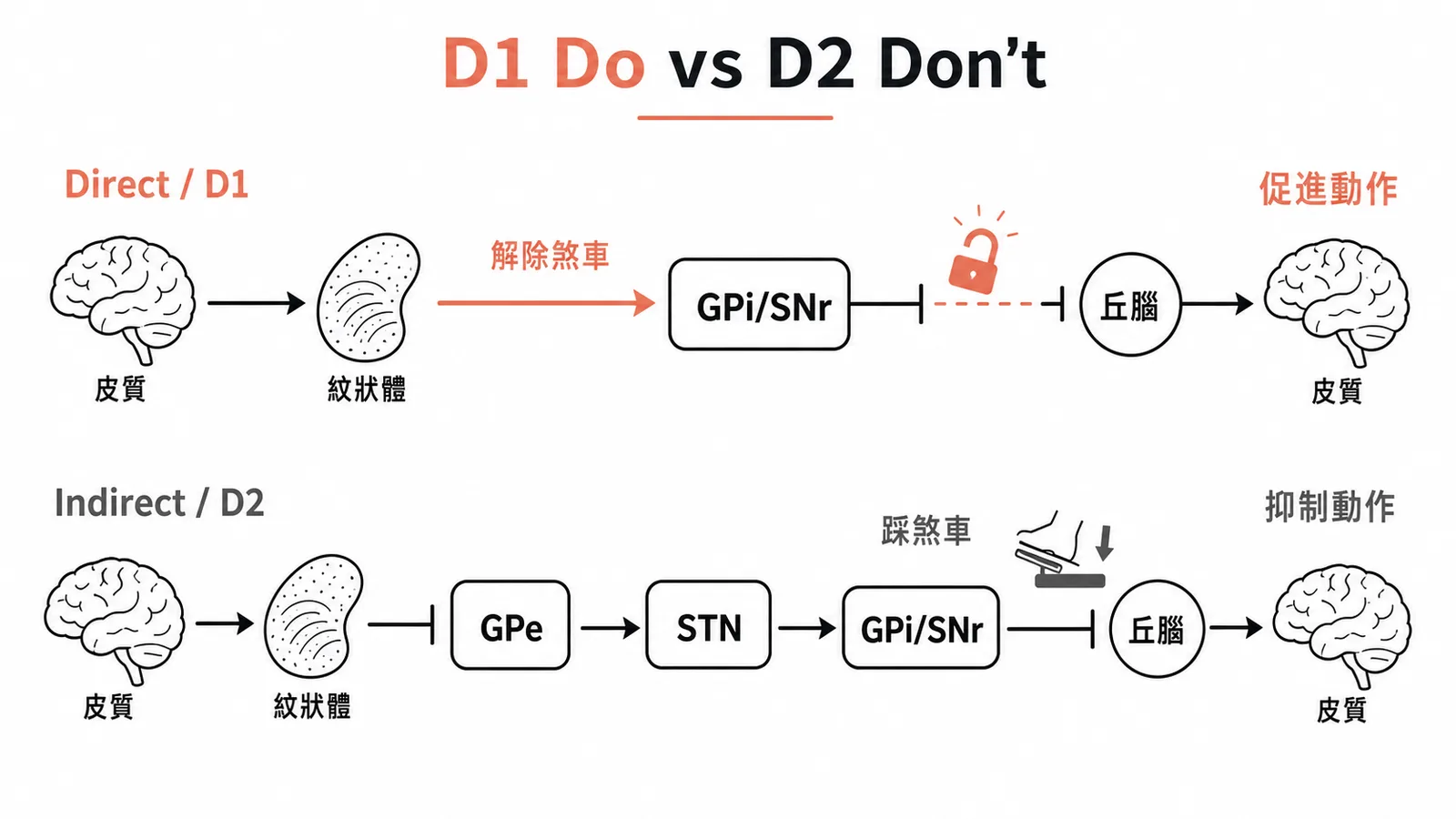
- 基底核 direct pathway 走 D1 receptor,解除丘腦抑制、促進動作;indirect pathway 走 D2,加強抑制、踩煞車。Parkinson's 是 SNc 多巴胺不夠 → indirect 過強 → bradykinesia;Huntington's 早期是 indirect 神經元先死 → direct 過強 → chorea。
- Hemiballismus 幾乎 100% 考 subthalamic nucleus(STN)損傷,原因是 lacunar stroke。STN 壞掉 → indirect pathway 的煞車失效 → 對側猛烈甩動。
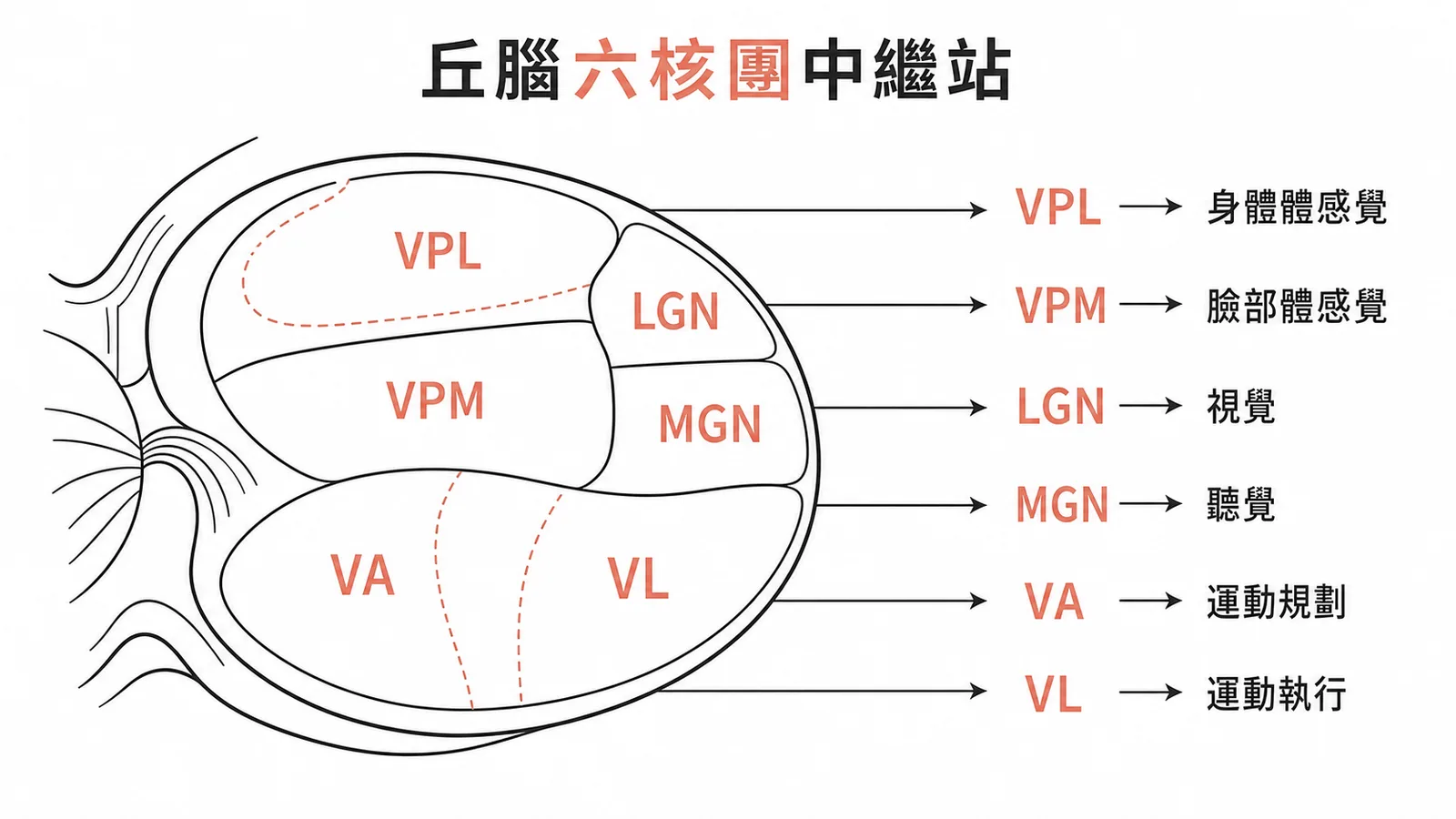
- 丘腦核團對照是高頻題:VPL 接身體體感覺(medial lemniscus + spinothalamic),VPM 接臉(trigeminal),LGN 接視覺,MGN 接聽覺,VA/VL 接基底核和小腦的運動輸出到皮質。
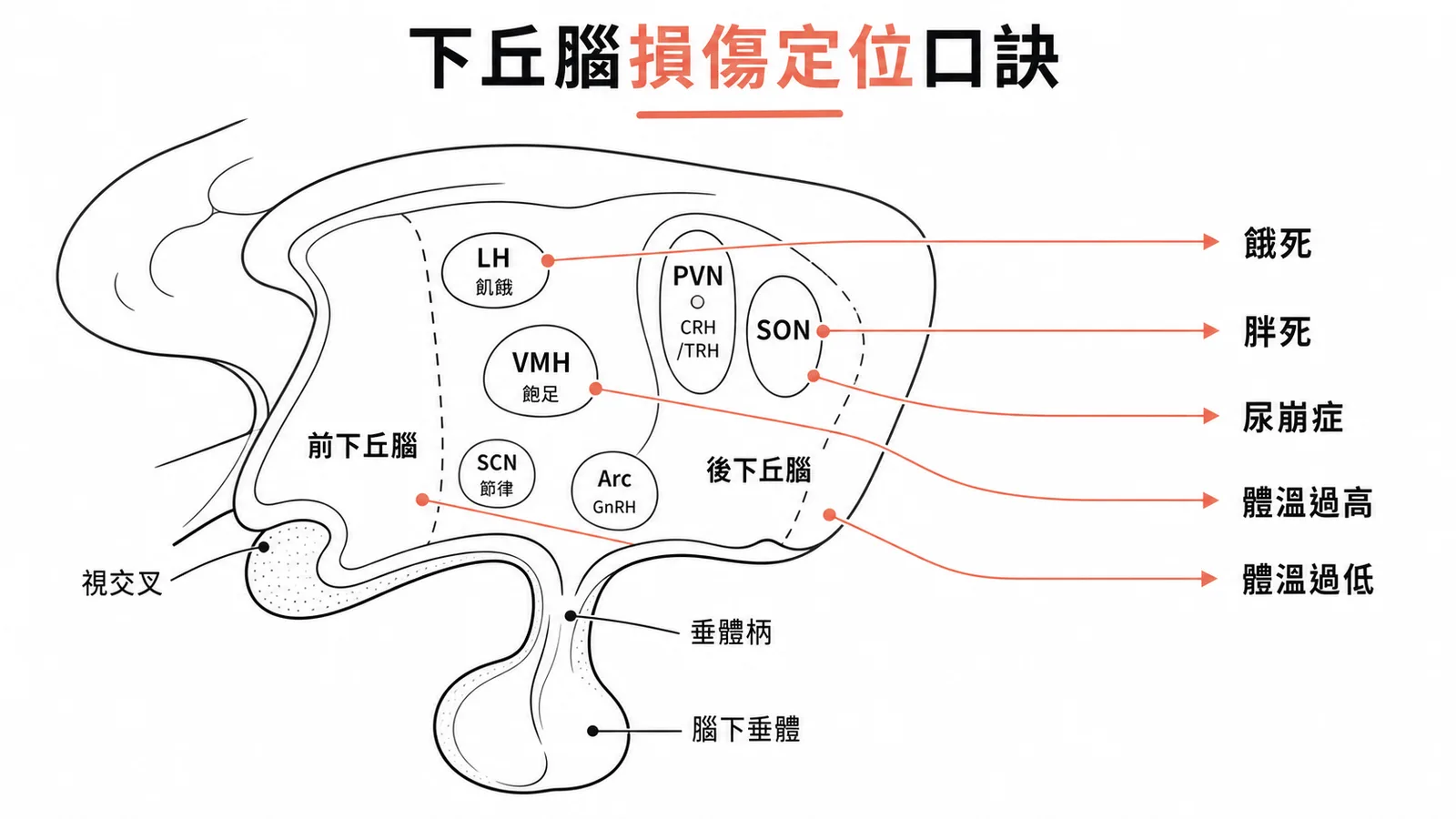
- 下丘腦損傷定位:lateral → 不吃(anorexia),ventromedial → 吃不停(obesity);supraoptic → ADH 缺乏(central DI);anterior → 散熱壞了(hyperthermia),posterior → 產熱壞了(hypothermia + somnolence)。
- Papez circuit 考 Korsakoff syndrome:酒精 → thiamine 缺乏 → mammillary body 壞死 → 嚴重 anterograde amnesia + confabulation。
- Kluver-Bucy syndrome = 雙側杏仁核損傷 → hyperorality + hypersexuality + visual agnosia + 情緒遲鈍。常出在顳葉切除或 HSV encephalitis 後。
- 內囊(internal capsule)後肢帶 corticospinal 和 corticobulbar tract,MCA 的紋狀體動脈(lenticulostriate arteries)和前脈絡叢動脈(anterior choroidal artery)供血。小血管梗塞 → 對側偏癱(pure motor hemiparesis)。
記憶口訣
- 「LH 餓死、VMH 胖死」— Lateral Hypothalamus 損傷不吃,Ventromedial 損傷吃不停。
- 「前冷後熱」— Anterior hypothalamus 管散熱(A/C = Air Conditioning),Posterior 管產熱保溫。
- 「D1 Do, D2 Don't」— Direct pathway 接 D1 促動作,Indirect 接 D2 踩煞車。
- 「VPL 四肢、VPM 臉嘴」— VPL 的 L 想成 Limbs(身體),VPM 的 M 想成 Mouth(臉部)。
- 「LGN 看 Light、MGN 聽 Music」— Lateral Geniculate 管視覺,Medial Geniculate 管聽覺。
- 「海馬穹窿乳頭丘腦扣帶」— Papez circuit 走法:Hippocampus → Fornix → Mammillary body → Anterior thalamus → Cingulate gyrus → Entorhinal cortex → 回到 Hippocampus。
大腦(cerebrum)和間腦(diencephalon)合稱前腦(prosencephalon),包含大腦皮質、基底核、丘腦、下丘腦和邊緣系統。
這些結構負責意識、語言、運動規劃、感覺整合、情緒和內分泌調控,是國考神經解剖出題的核心區域。
大腦皮質功能定位
大腦皮質的每個區域有特定功能,損傷位置不同就會出現不同的臨床症狀。
初級運動皮質(primary motor cortex, Brodmann area 4)在中央前回(precentral gyrus),控制對側身體的隨意動作。皮質上有 somatotopic organization——臉和手占的面積最大(精細動作多),下肢的代表區在大腦縱裂的內側面。
初級感覺皮質(primary somatosensory cortex, BA 3, 1, 2)在中央後回(postcentral gyrus),接收對側身體的觸覺、本體感覺、痛覺和溫度覺,同樣有體部位對應排列。
Broca's area 在優勢半球(通常左側)的下額回(inferior frontal gyrus, BA 44, 45),負責語言的「產出」——組織語句、驅動說話的運動程序。
損傷後出現 Broca's aphasia:聽得懂別人說什麼,但自己說不出流暢的句子(non-fluent aphasia),說話費力、電報式。
Wernicke's area 在優勢半球的後上顳回(posterior superior temporal gyrus, BA 22,延伸至 39, 40),負責語言的「理解」——解碼聽到的語音。
損傷後出現 Wernicke's aphasia:說話流利但內容錯亂無意義(fluent aphasia),病人不自覺有問題,常出現 neologism(自創詞)。
連接 Broca's 和 Wernicke's 的白質纖維束是弓狀束(arcuate fasciculus)。損傷造成 conduction aphasia:聽得懂、也能說,但「覆述」(repetition)特別差。
基底核與運動迴路
基底核(basal ganglia)是埋在大腦深處的一群灰質核團,負責調控動作的啟動和抑制。
主要成員包括尾核(caudate nucleus)、殼核(putamen)、蒼白球(globus pallidus)、黑質(substantia nigra)和丘腦下核(subthalamic nucleus, STN)。
尾核加殼核合稱紋狀體(striatum),是基底核的「輸入站」——接收大腦皮質送來的訊號。蒼白球內段(GPi)和黑質網狀部(SNr)是「輸出站」,把處理結果送往丘腦。
Direct pathway(直接通路)走 D1 receptor:皮質 → 紋狀體 → 直接抑制 GPi/SNr → GPi/SNr 對丘腦的抑制減弱 → 丘腦活化 → 促進動作。簡單說就是「解除煞車」讓動作發生。
Indirect pathway(間接通路)走 D2 receptor:皮質 → 紋狀體 → GPe → STN → 加強 GPi/SNr 的輸出 → 丘腦抑制增強 → 動作被壓制。這條路是「踩煞車」。
黑質緻密部(SNc)釋放多巴胺到紋狀體,同時興奮 D1(促直接通路)和抑制 D2(壓間接通路),淨效果是促進動作。
Parkinson's disease 的核心病理是 SNc 多巴胺神經元退化。多巴胺不夠 → direct pathway 活性下降 + indirect pathway 過度活化 → bradykinesia(動作慢)、rigidity(僵直)、resting tremor(靜止性震顫)、postural instability(姿態不穩)。
Huntington's disease 是紋狀體的中型棘突神經元(medium spiny neurons)退化,跟 CAG trinucleotide repeat expansion 有關。早期先死掉的是 indirect pathway 的神經元 → 煞車失靈 → direct pathway 相對過強 → chorea(舞蹈症)。晚期 direct pathway 也退化,動作反而變慢變僵。
Hemiballismus 是 STN 損傷(通常是 lacunar stroke)。STN 本來負責驅動 indirect pathway 的煞車,壞掉後煞車失效 → 對側肢體出現猛烈的甩動(flinging)動作。
內囊(internal capsule)位在丘腦/尾核和豆狀核之間的白質帶,後肢帶 corticospinal tract 和 corticobulbar tract,是運動訊號從皮質到腦幹和脊髓的必經之路。供血來源包括 MCA 的紋狀體動脈(lenticulostriate arteries)和前脈絡叢動脈(anterior choroidal artery)。小血管梗塞造成對側偏癱,是 lacunar stroke 最常見的表現之一。
丘腦中繼核與皮質投射
丘腦(thalamus)是幾乎所有感覺訊號(嗅覺除外)進入大腦皮質前的最後一站。不同的核團負責中繼不同類型的訊息。
VPL(ventral posterolateral nucleus)接收來自身體的體感覺。輸入來源是內側蹄系(medial lemniscus,傳精細觸覺和本體感覺)和脊髓丘腦徑(spinothalamic tract,傳痛覺和溫度覺),投射到中央後回的體感覺皮質。
VPM(ventral posteromedial nucleus)接收來自臉部的體感覺。輸入是三叉神經徑路(trigeminal pathway),投射到體感覺皮質的臉部代表區。
LGN(lateral geniculate nucleus)是視覺的中繼站。接收視網膜的訊號(經 optic tract),投射到初級視覺皮質 V1(Brodmann area 17,枕葉距狀裂 calcarine cortex)。
MGN(medial geniculate nucleus)是聽覺的中繼站。接收下丘(inferior colliculus)的訊號,投射到初級聽覺皮質 A1(上顳回)。
VA(ventral anterior nucleus)接收基底核輸出(GPi、SNr)的訊號,投射到前運動皮質和輔助運動區(SMA)。
VL(ventral lateral nucleus)接收 GPi/SNr 的訊號,也接收小腦深層核(deep cerebellar nuclei)的輸入,投射到初級運動皮質和前運動皮質。
一句話分清楚:感覺走 VP 系列和膝狀體(VPL/VPM/LGN/MGN),運動走 VA/VL。小腦的運動校正訊號也透過 VL 到達運動皮質。
丘腦前核(anterior nucleus)接收乳頭體經乳頭丘腦徑(mammillothalamic tract)的投射,是 Papez circuit 的一環,參與記憶和情緒處理。
下丘腦核團與功能
下丘腦(hypothalamus)體積很小,不到全腦的 1%,但管的事情很多:自主神經、內分泌、體溫、食慾、睡眠、情緒。
外側下丘腦(lateral hypothalamus)是飢餓中樞,促進食慾和維持清醒。損傷後動物不吃不喝(anorexia),消瘦而死。
腹內側下丘腦(ventromedial hypothalamus, VMH)是飽足中樞,感應「吃飽了」的訊號。損傷後停不下來一直吃(hyperphagia),變得極度肥胖。
視交叉上核(suprachiasmatic nucleus, SCN)是生理時鐘的主節律器。接收視網膜光線訊號,輸出到松果體調控 melatonin 分泌,建立 24 小時的晝夜節律(circadian rhythm)。
視上核(supraoptic nucleus)合成 vasopressin(ADH)和 oxytocin,沿軸突運送到腦下垂體後葉(posterior pituitary)釋放。損傷造成中樞性尿崩症(central diabetes insipidus)——排出大量稀釋尿液、血鈉上升。
室旁核(paraventricular nucleus)也合成 vasopressin 和 oxytocin,同時製造 CRH 和 TRH,經正中隆起(median eminence)釋放到垂體門脈系統,調控腎上腺和甲狀腺軸。
弓狀核(arcuate nucleus)製造多巴胺(抑制泌乳素分泌)、GnRH、GHRH,以及控制食慾的兩組拮抗訊號——POMC/α-MSH 抑制食慾,NPY/AgRP 促進食慾。
前下丘腦(anterior hypothalamus)負責散熱反應——血管擴張、出汗——也管副交感功能。損傷後身體無法散熱,導致高體溫(hyperthermia)。
後下丘腦(posterior hypothalamus)負責產熱保溫——顫抖、血管收縮——也透過釋放組織胺維持清醒。損傷後無法產熱,導致低體溫(hypothermia)加上嗜睡(somnolence)。
邊緣系統與記憶迴路
邊緣系統(limbic system)是環繞在胼胝體周圍的一組結構,負責情緒、記憶和動機行為。主要成員包括海馬迴(hippocampus)、杏仁核(amygdala)、扣帶回(cingulate gyrus)、乳頭體(mammillary body)和隔區(septal area)。
Papez circuit 是最經典的記憶迴路:海馬迴 → 穹窿(fornix)→ 乳頭體 → 乳頭丘腦徑(mammillothalamic tract)→ 丘腦前核 → 扣帶回 → 扣帶束(cingulum)→ 內嗅皮質(entorhinal cortex)→ 回到海馬迴。
這條環路對記憶鞏固(consolidation)和情緒處理都很關鍵。環路上任何一點損傷都可能造成前向失憶(anterograde amnesia)。
最典型的例子是 Korsakoff syndrome:長期酒精濫用 → thiamine(B1)缺乏 → 乳頭體和丘腦背內側核壞死 → 嚴重前向失憶加虛構記憶(confabulation)。通常緊接在 Wernicke encephalopathy(急性混亂、眼肌麻痺、步態不穩)之後。
海馬迴接收內嗅皮質經穿通路徑(perforant pathway)送來的訊號,經過三突觸迴路(trisynaptic circuit)處理:內嗅皮質 → 齒狀回(dentate gyrus)→ CA3 → CA1 → 海馬下托(subiculum)。輸出經穹窿投射到乳頭體、隔區和丘腦前核。
海馬迴是形成陳述性記憶(declarative memory)的關鍵結構。雙側損傷會造成嚴重的前向失憶——記不住新事物,但已鞏固在皮質的舊記憶通常保留。
杏仁核(amygdala)是情緒記憶和恐懼制約(fear conditioning)的核心,有兩條主要的傳出路徑。
終紋(stria terminalis)從杏仁核的內側和中央核出發,投射到下丘腦、終紋床核(bed nucleus of stria terminalis, BNST)和隔區,調控情緒刺激引起的自主神經和內分泌反應。
腹側杏仁逃逸徑(ventral amygdalofugal pathway)從基底外側核出發,擴散投射到下丘腦、丘腦、伏隔核(nucleus accumbens)和前額葉皮質,負責情緒學習、恐懼制約和獎賞處理。
雙側杏仁核損傷會出現 Kluver-Bucy syndrome:什麼都放嘴巴(hyperorality)、性行為失控(hypersexuality)、看到東西卻認不出意義(visual agnosia)、情緒反應遲鈍。最常見的病因是雙側顳葉損傷,例如 HSV encephalitis 好犯顳葉,術後或感染後都可能出現。
臨床損傷定位總整理
| 損傷部位 | 臨床表現 | 考題線索 |
|---|---|---|
| Broca's area(左下額回 BA 44, 45) | Non-fluent aphasia:聽懂但說不出 | 電報式語言、病人挫折感強 |
| Wernicke's area(左後上顳回 BA 22) | Fluent aphasia:說流利但胡言亂語 | Neologism、不自覺有問題 |
| 弓狀束(arcuate fasciculus) | Conduction aphasia:覆述特差 | 聽得懂也能說,repeat 困難 |
| SNc(黑質緻密部) | Parkinson's disease | Bradykinesia + rigidity + resting tremor |
| 紋狀體(indirect pathway 先退化) | Huntington's disease | Chorea + CAG repeat + 家族史 |
| STN(丘腦下核) | Hemiballismus:對側猛烈甩動 | Lacunar stroke、急性發作 |
| 內囊後肢 | 對側 pure motor hemiparesis | Lacunar stroke |
| Mammillary body | Korsakoff syndrome | 酒精史、thiamine 缺乏、confabulation |
| 雙側海馬迴 | 嚴重前向失憶 | 新記憶不能形成、舊記憶保留 |
| 雙側杏仁核 | Kluver-Bucy syndrome | Hyperorality + hypersexuality |
| Lateral hypothalamus | Anorexia、消瘦 | 拒食 |
| Ventromedial hypothalamus | Hyperphagia、肥胖 | 吃不停 |
| Supraoptic / paraventricular nucleus | Central diabetes insipidus | 多尿、低比重尿、高血鈉 |
| Anterior hypothalamus | Hyperthermia | 無法散熱 |
| Posterior hypothalamus | Hypothermia + somnolence | 無法產熱、嗜睡 |